|
Fluorescein Angiography For Beginners |
Dr Sudhir
Singh, M.S.
Consultant Ophthalmologist
J.W.Global Hospital & Research Centre, Mount Abu.
India.307501
https://sudhir.info/
|
|
Introduction
Fluorescein angiography
is a fundal photography, performed in rapid sequence
following intravenous injection of fluorescein dye.
It provides following information’s:
1.
The blood flow
characteristics in the vessels as the dye reaches
and circulates through the retina and choroid
2.
It provides fine details
of the retinal circulation and pigment epithelium
that may not otherwise be visible.
3.
It records functional
integrity
retinal vessels, so their assessment can be done.
Fluorescein
-
Sodium
fluorescein is an organic dye.
-
Sodium
fluorescein (C20H10O5Na2) has molecular weight of
376 Daltons.
-
It is
80% bound to plasma albumin. The remaining 20% is
seen during angiography
-
The
Sodium fluorescein absorbs light in the blue range
of the visible spectrum, with absorption peaking at
490nm (blue). It emits light at 530nm (yellow).
-
It is
metabolized by the liver and excreted by the
kidneys. Most dye is cleared with 24 hours and
patients should be warned that their urine will
appear orange during this time.
|
|
|
|
|
Physiology
There
are two circulations within the fundus:
a.
Choroidal circulation
-
The fluorescein freely leaks out of the fenestrated
choroidal capillaries, and from there through
Bruch's membrane. However, tight junctions between
retinal pigment epithelium (RPE) cells prevent dye
reaching the retina.
b.
Retinal circulation
-
The retinal blood vessel endothelial cells are
joined by tight junctions which prevent leakage of
fluorescein into the retina. This constitutes the
blood retina barrier. Any leakage from the retinal
vessels is considered as an abnormal.
Fluorescein cannot diffuse through tight cellular
junctions. These are present at two sites within the
fundus:
1.
Retinal blood vessel endothelium
2.
Retinal pigment epithelium.
|
|
|
Phases Of Fluorescein Angiography
n
Choroidal phase
- Choroidal filling via the short ciliary arteries
results in initial patching filing of lobules, very
quickly followed by a diffuse (blush) as dye leaks
out of the choroidocapillaris. Cilioretinal vessels
and prelaminar optic disc capillaries fill during
this phase
n
Arterial
phase - The central retinal artery fills about 1
second later than choroidal filling. So dye is only
visible in central retinal artery but not in retinal
veins.
n
Capillary
phase- The capillaries quickly fill following
the arterial phase. The perifoveal capillary network
is particular prominent as the underlying choroidal
circulation is masked by luteal pigment in the
retina and melanin pigment in the RPE. At the centre
of this capillary ring is the foveal avascular zone
500um in diameter
n
Venous
phase
- Early filling of the veins is from tributaries
joining their margins, resulting in a tramline
effect. Later the whole diameter of the veins is
filled.
n
Late
phase
- After 10 to 15 minutes little dye remains within
the blood circulation. Dye which has left the blood
to ocular structures is particularly visible during
this phase.
|
|

Arteial Phase |

Early Venous Phase |

Late Venous Phase |
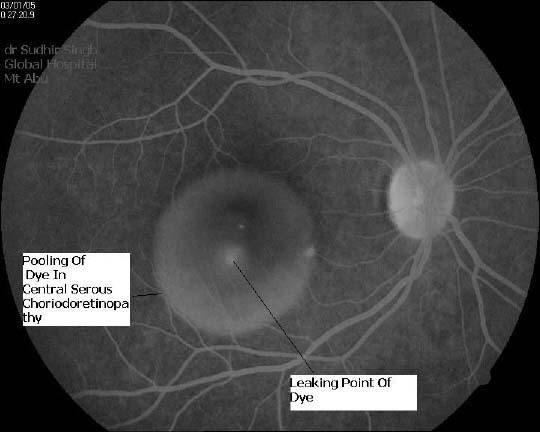
Pooling of dye in CSR(Central
Serous Choroidoretinopathy). |

Hyper-fluorescence and
Hypo-fluorescence (Courtsey: Dr Sudhir Singh) |
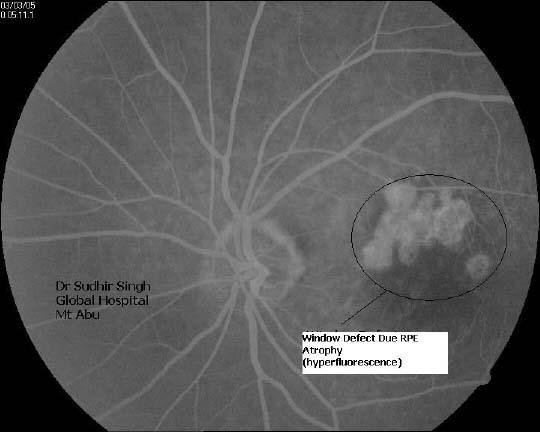
Window defect due to RPE atrophy
(Courtsey: Dr Sudhir Singh) |

Dye leaking neo vascularization
and aneurysms,Venous beading(Courtsey: Dr Sudhir
Singh) |
|
|
Procedure
n
The
patient is advice to sit in front of fundus camera
comfortably and take explained written consent.
n
The
central retina is focused with fundus camera.
n
One
coloured fundus photograph of each eye taken before
injecting dye.
n
One
photograph of each fundus also taken with exciter
filter in place to record pseudo fluorescence and
auto fluorescence.
n
5ml of
10% sodium fluorescein dye is injected as a bolus
into the vein (preferably antecubital) of the
patient's arm or in any other vein of forearm with
the help of scalp vein set.
n
The
blue filter (excitation filter) of fundus camera
turned on. The fundus is viewed through a yellow
filter (barrier filter). As blue light cannot pass
through a yellow filter in normal circumstances
nothing can be seen. However, fluorescein dye within
retinal and choroidal blood vessels absorbs blue
light and emits yellow light; this yellow light
passes through the filter and is photographed. Only
tissues that contain fluorescein are visualized.
n
An
initial exposure rate of 1 frame (snap) every few
seconds (5 seconds) documents the arteriolar and
early venous filling phase of the study. Exposures
are then made at less frequent intervals until 20 to
25 frames are exposed. Late phase photograph are
taken after a pause of 10to 30 minutes.
|
|
|
Side Effects
-
Nausea and vomiting (10%). Bowl should be kept ready and
patient should assused, this is usually subsides without any
medication.
-
Vasovagal syncope (1%) and no treatment is needed. But in
extreme bradycardia, IV atropine (0.6mg).
-
Anaphylaxis such as bronchospasm, urticarial skin rash and
hypotension (<1%). Treatment is with chlorpheniramine (Avil)
10mg IV, hydrocortisone 100mg IV and give oxygen and
adrenaline 1ml of 1:1000 SC/IM for hypotension and
bronchospasm.
-
Cardiac and respiratory arrest (<0.01%). Treatment would
involve cardiopulmonary resuscitation.
-
Temporary tan skin colour from the dye. Patient should be
assured
-
Discoloration of the urine. Patient should be assured.
|
|
Analysis Of Fluorescein Angiogram
Sequential analysis :
It is examined frame by frames in the order that it
was photographed. The major vascular phases of the
angiogram are emphasized. This method is most useful
in analyzing vascular disorders of the retinal and
choroidal.
Anatomic analysis :
Observes each of the major layers of the posterior
pose of the eye - the choroidal,
RPE and neurosensory retina.
Morphologic analysis
:
Considers overall patterns. In an abnormal
angiogram, some areas may be darker (hyper
fluorescent) or lighter (hypo fluorescent) than
usually in a given location.
Hypo
fluorescence is caused by following
Transmission Defect
is caused by pre or intra retinal haemorrage,
pigment, hard and soft exudates etc
Filling Defect
is
caused by circulation abnormality like CRAO, CRVO
and BRVO and non perfusion due capillary dropout.
|
|
Indications of Fluorescein Angiography
-
Age related macular degeneration.
-
Cystoid macular edema.
-
Neovascularizations.
-
Diabetic retinopathy.
-
Central
serous choroidoretinopathy.
-
Artery and vein occlusion.
-
Retinal Inflammations
-
Tumours.
|
 |
 |
|
Hyper
fluoresence is caused following factors:
1. Window
Defect (RPE Defect) :
This is an increase in fluorescence caused by a disruption
in the continuity of the RPE layer. The view of the
normal choroidal vessel leakage through a break in the
retinal pigment layer. the de-pigmentation seen in
some macular scars is a common example of window
defect.
2. Leakage
of Dye :
The fluorescein does not leak from normal retinal vessels.
The leakage is either due to loss retinal vascular
endothelial tight junction (e.g. diabetic retinopathy) or
from the loss of RPE (e.g. central serous chorioretinopathy)
or across Bruchs’ membrane ( e.g. PED and drusen).
3. Pooling
of Dye () : The
pooling occurs when leaking dye collects in a sub-retinal
space. Examples ;
RPE Detachment and
central serous chorioretinopathy.
4. Staining
of Dye: The
Staining occurs when tissue absorbs fluorescein dye. The
example of abnormal staining occurs in the tissue of a
malignant melanoma and drusen.
5. Auto
Fluorescence : The
Auto-fluorescence occurs
when a highly reflective structure, such as optic nerve head
drusen, is seen when photographed prior to the injection of
fluorescein.
|